A 78 year old patient with complaints of pedal edema shortness of breath
MARCH 8TH 2022
This is an E log book to discuss our patients deidentified health data shared after guardians informed consent.
here we discuss our individual patient problems through series of inputs from available global online community of experts with an aim to solve this patients clinical problems with collective current best evidence based inputs.
This E-book also reflects my patients centered online learning portfolio and your valuable comments in comment box are most welcome.
I have Been given this case to solve in an attempt to understand the topic of "patient clinical data analysis"to develop my competency and comprehending clinical data including history,clinical finding investigations and come up with a diagnosis and treatment plan.
MARCH 8TH 2022
CASE
A 78 year old patient came with chief complains of
1. shortness of breath since 3 months
2. pedal edema since 3 months
3. chest pain- intermittent since 15 days.
HISTORY OF PRESENTING ILLNESS:
Patient was apparently asymptomatic 3 months back, then he developed exertional dyspnea associated with cough( wet type-sputum).
there is also H/O bilateral pedal edema which is of pitting type(Grade 1) since 3 months. facial puffiness also seen.
H/O chest pain intermittent since 15 days.
No H/O fever, burning micturition, palpitation, decreased urine output.
PAST HISTORY:
PERSONAL HISTORY:
FAMILY HISTORY:
GENERAL EXAMINATION:
Patient is conscious, coherent and cooperative, well oriented to time, place, person.
Thin built moderately nourished
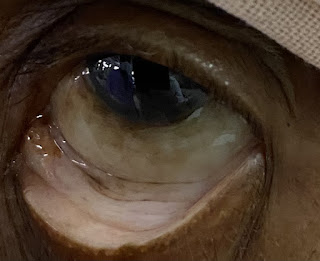
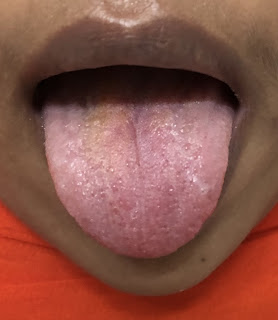
Pallor- present
Icterus- absent
Cyanosis- absent
clubbing- absent
Lymphadenopathy- absent
Edema- present





VITALS:
SYESTEMIC EXAMINATION:
INVESTIGATIONS:
ECG:

2-D ECHO:

USG:

MARCH 9th 2022



HEART FAILURE WITH PROLONGED EJECTION FRACTION DIAGNOSED AS CHRONIC RENAL FAILURE ASSOCIATED WITH HYPERTENSION
1. FLUID RESTRICTION < 1.5 LT/DAY
2. SALT RESTRICTION < 2 GM /DAY
3. TAB. LASIX 40 MG / BD
4. TAB. NICARDIA 10 MG / BD
5. TAB. NODOSIS 500 MG / BD
6. TAB. SHELCAL 500 MG / OD
7. CAP. BIO D3 0.25 MG / OD
8. TAB. OROFER XT / BD
9. INJ. IRON SUCROSE 100 MG IN 100 ML NS / IV OVER 1 HR
10. INJ. ERYTHROPOIETIN 4000 U/ SC X ONCE WEEKLY
11. TAB. MET XL 12.5 MG / OD


Comments
Post a Comment